
Pediatric MRI introduces unique safety challenges.
Understanding these risks — and managing them through structured workflows, communication, and careful patient positioning — is essential for safe and successful imaging.
Stephen Mercedes MBA, BHA, MRSO, RT(R)(MR)
Content
1. WHY PEDIATRIC MRI SAFETY REQUIRES SPECIAL ATTENTION
2. SPECIAL RISK FACTORS IN PEDIATRIC MRI
3. THE COMPLEXITY OF PERSONNEL IN PEDIATRIC MRI
4. SEDATION AND ANESTHESIA
5. COMMUNICATION WITH PEDIATRIC PATIENTS
6. SPECIAL CASES: FEED-AND-SWADDLE EXAMINATIONS
7. RECOMMENDATIONS
8. Conclusion
SOURCES
1. Why Pediatric MRI Safety Requires Special Attention
Magnetic Resonance Imaging (MRI) is one of the most powerful diagnostic tools in modern medicine. At the same time, it is one of the most complex clinical environments in terms of safety. Strong magnetic fields, radiofrequency energy, and rapidly switching gradients create risks that are invisible but constantly present.
While these challenges exist in every MRI department, they become significantly more complex when imaging pediatric patients. Children often require additional support to remain still during examinations, and pediatric MRI frequently involves sedation, anesthesia, or specialized preparation techniques.
For radiology teams, this means that safety in pediatric MRI extends beyond standard MRI protocols. It requires coordinated teamwork, clear communication, structured workflows, and careful patient positioning to ensure both safety and diagnostic image quality.
2. Special Risk Factors in Pediatric MRI
Pediatric MRI environments differ from adult imaging in several important ways. Two of the most significant factors are the complexity of the clinical team present in the MRI environment and the frequent need for sedation or anesthesia.
Together, these factors increase the complexity of maintaining a safe MRI environment and place additional responsibility on MRI technologists to ensure that safety protocols are consistently followed.
3. The Complexity of Personnel in Pediatric MRI
MRI departments are often physically separated from other hospital areas and may operate in enclosed spaces without direct visibility from other clinical teams. For many non-radiology staff members, the MRI department is simply known as a restricted area due to the strong magnetic field.
In adult MRI departments, staffing typically consists of one MRI technologist per scanner with occasional additional support staff. Pediatric MRI environments, however, often involve a much larger multidisciplinary team.

One dramatic moment showing every type of individual who can be in a pediatric MRI department at the same time — all gathered together in the controlled Zone 3 area
At any given time, personnel present in a pediatric MRI department may include:
- MRI technologists — managing the scanner and imaging protocols
- Sedation nurses & physicians — ensuring safe sedation for young or anxious patients
- Respiratory therapists & nurse anesthetists — monitoring and supporting breathing
- Anesthesiologists — overseeing complex sedation cases
- Medical physicists — maintaining safety and image quality standards
- Medical or technical assistants — supporting clinical workflows
- Child Life specialists — helping children and families cope with the experience
- Floor nurses — accompanying patients from their ward

The 10 key personnel roles typically present in a pediatric MRI department
Additional individuals may also enter the environment, including engineering staff, environmental services personnel, radiology leadership, and parents accompanying the child.
The presence of many individuals in the MRI environment increases the complexity of maintaining safety. MRI technologists therefore play a central role in ensuring that every individual entering controlled areas has been properly screened for implants, devices, and external metallic items before entering Zones 3 and 4.

MRI technologist as safety gatekeeper — all staff and visitors must be screened before entering Zones 3 & 4
4. Sedation and Anesthesia
Remaining motionless for 30–45 minutes inside a narrow scanner with noise levels exceeding 100 decibels can be extremely challenging for young patients. To enable successful imaging, different levels of sedation may be used, including:
-
minimal sedation (e.g., nitrous oxide or intranasal medication)
-
moderate sedation (e.g., oral medication or intravenous analgesia)
-
deep sedation (e.g., IV propofol or fentanyl)
-
general anesthesia
Under sedation, patients may still respond to external stimuli. Under general anesthesia, however, patients become fully dependent on monitoring equipment and clinical staff to maintain breathing and vital functions.
In these situations, sedation or anesthesia teams are primarily focused on maintaining the patient’s vital signs before, during, and after the examination. MRI safety considerations may therefore not always be their primary focus.
As a result, MRI technologists remain responsible for ensuring that all equipment entering the scanner room is MRI-compatible and that safety protocols are maintained throughout the procedure.
Sedated or anesthetized patients also introduce another safety consideration: they cannot communicate discomfort during the scan. If heating or pressure occurs during imaging, the patient may not be able to report it.
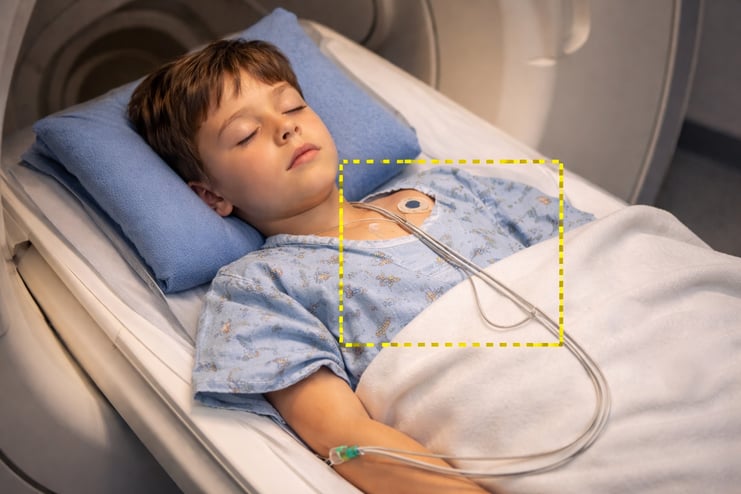
A child inside an MRI scanner with monitoring cables on the chest. The highlighted cables show a critical safety concern: in sedated patients, the inability to communicate discomfort means worn or improperly positioned cables may overheat and cause (RF) burns.
For this reason, careful patient positioning and insulation become even more critical during these examinations. Preventing skin-to-skin contact, avoiding contact with the bore, and ensuring proper padding can significantly reduce the risk of radiofrequency (RF) burns.
Although RF injuries are rare, they remain one of the most commonly reported MRI-related injuries. In a reported case from 2024, a patient experienced a heating sensation during imaging that was initially ignored, later resulting in a stage III burn (Abu-Shanab et al., 2025). For sedated patients, such early warning signs cannot be communicated, making preventive measures even more important.
5. Communication with Pediatric Patients
Not every pediatric MRI exam requires sedation. In many cases, effective communication can significantly improve patient cooperation and reduce the need for medication.
Preparation often begins before the patient arrives in the MRI department. Parents, Child Life specialists, and MRI teams can work together to prepare children for the examination at home.
With structured preparation programs, some institutions have achieved remarkable results. For example, the New York-based Hospital for Special Surgery (2023) reported a 0% sedation rate in nearly 2,000 pediatric MRI examinations through targeted preparation, patient education, and support by Child Life specialists.
On the day of the examination, MRI technologists play a key role in guiding pediatric patients through the process. Successful strategies may include:
-
clearly explaining expectations to both the child and parent
-
performing practice runs or demonstrations
-
pausing the examination when reassurance is needed
-
adapting communication to the child’s age and personality
Children between six and fourteen years of age can respond very differently to medical procedures. Some may prefer clear instructions and reassurance, while others may want to understand every step of the process. Meeting pediatric patients at their level is often the key to successful imaging.
6. Special Cases: Feed-and-Swaddle Examinations
One specialized pediatric MRI technique is the feed-and-swaddle (also known as feed-and-wrap) method, typically used for infants up to approximately six months of age.
Parents are usually asked to delay feeding prior to the exam and then feed the infant immediately before scanning. The goal is to allow the infant to fall asleep naturally during the examination.
The infant is then carefully swaddled or immobilized before scanning begins. Timing is critical, as longer preparation times increase the likelihood that the infant will wake before the exam is completed.

Feed-and-swaddle: A mother holds her infant right before placing them into the MRI scanner
These examinations require efficiency and coordination from the MRI technologist. The shorter the setup and scanning time, the greater the chance of completing the exam successfully while the infant remains asleep.
Another important safety consideration is the risk of aspiration. Infants may not be able to clear their airway effectively if milk or formula enters the airway. Monitoring systems such as pulse oximetry are therefore commonly used to track vital signs throughout the examination.
7. Recommendations
In conclusion there are many different facets to safety considerations in pediatric MRI. Some of those facets not mentioned that we will further cover in later posts include protocol management (as protocols require very specific adjustments for children), effective screening methods, implant/device safety measures, proper emergency management procedures and much more.
Below are my recommendations and summary for the earlier points mentioned. These recommendations are designed to promote safe practices and align with Uramatsu et al., their article Improving Pediatric Magnetic Resonance Imaging Safety by Enhanced Non-Technical Skills and Team Collaboration, where they state, “Strengthening collaboration, refining sedation protocols, and implementing advanced safety monitoring systems are essential steps” (2025).
Personnel and Safety
Implement comprehensive screening for patients and staff, enforce MRI zone restrictions with clearly defined clearance levels, utilize ferromagnetic detection systems (FDMS), and conduct standardized safety time-outs prior to scanning.
Sedation and Anesthesia
Ensure all equipment is MRI-compatible and properly secured, remove unsecured supplies before room entry, and adhere strictly to established safety time-out protocols.
Communication and Patient Preparation
Incorporate mock scanner training when appropriate, assess preferred communication methods, pause imaging as needed for patient reassurance, and collaborate with Child Life specialists to optimize patient cooperation.
Feed-and-Swaddle Examinations
Provide clear timelines and expectations to parents, use protective padding as needed, maintain appropriate scanner ventilation, minimize unnecessary materials in the bore, and reduce idle time to limit infant movement.
8. Conclusion
Pediatric MRI presents unique safety challenges that extend beyond standard imaging procedures. The presence of multidisciplinary teams, the frequent use of sedation or anesthesia, and the complexity of imaging infants require careful coordination and heightened awareness.
Ensuring safety in pediatric MRI depends on strong teamwork, structured workflows, and consistent safety protocols. Clear communication between radiology staff, anesthesia teams, and caregivers plays a critical role in reducing risk.
By combining well-defined safety procedures with thoughtful patient preparation and careful positioning practices, MRI teams can significantly improve both patient safety and the overall quality of pediatric imaging.
Sources
Abu-Shanab, A., Nasr, H., Mohd, A., Shaweish, M., Abdulraheem, A., & Du, D. (2025). A rare case of MRI-induced thermal burn: Clinical implications and safety awareness. Radiology Case Reports, 20(5), 2243–2247. https://doi.org/10.1016/j.radcr.2025.01.064
Hospital for Special Surgery. (2023). HSS achieves 100% success rate for sedation-free pediatric MRIs. https://news.hss.edu/hss-achieves-100-success-rate-for-sedation-free-pediatric-mris/
Uramatsu, M., Takahashi, H., Barach, P., Fujisawa, Y., Takahashi, M., Mishima, S., & Yamanaka, G. (2025). Improving pediatric magnetic resonance imaging safety by enhanced non-technical skills and team collaboration. Brain and Development, 47(1), 104311. https://doi.org/10.1016/j.braindev.2024.104311